Miss S. is a 25-year-old female. Miss S. reported having been working in the modeling industry since the age of 8 years old. Miss S. stated that she has always been preoccupied with keeping a thin body frame and she reported having been on a diet “since ever”. When Miss S. was six years old she lost her mother due to heart disease. Miss S. reported that she used to look at her mother’s photos and was “disgusted” by her mother’s obese body shape. Miss S. reported that at the age of 8 she had to stay away from school to take care of her father who was hospitalized due to overweight-related problems. Miss S. stated that this became a turning point in his life as she started to idolize thin people.
Description of Presenting Problem
Ms. S. reported feeling apprehensive and unsure about her body image. Miss S. reported that she has always been obsessed with food. She stated that she rarely ate in public or presence of others. She reported ritualized food habits (cutting food into very small pieces, chewing for long period). Miss S. reported fainting on the stage while she was cut walking due to starvation and lack of energy.
Diagnosis
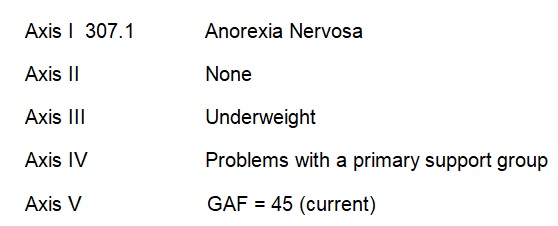
Based on the reported symptoms, Ms. S’ condition meets the DSM-IV TR criteria for 307.1 Anorexia Nervosa. The diagnosis was derived owing to a reported persistent fear of gaining weight, distorted and implacable attitudes toward food (self-inflicted starvation); distorted body image (believes she is always too fat).
Social psychology helps in understanding and explaining social behavior. Development psychology is concerned with human growth, development, and learning. In treating and understanding the problem, two theories can be used; these are cognitive theory and behavioral theory. The cognitive theory was developed by Aaron T. Beck in 1960. The cognitive theory outlines techniques used in treatment like rational analysis, double standard dispute, catastrophe scale, devil’s advocate, and reframing. The behavioral theory was advocated for by John B. Watson and B.K. Skinner in the early 1950’s. Behavioral techniques include exposure, shame attacking, risk-taking, postponing gratification, and stepping out of character.
Intervention – Cognitive-Behavioral Approach
One of the therapeutic interventions that can be used is rational emotive behavior therapy which teaches clients to unupset themselves and get empowered to lead happy life which is fulfilling (Ellis, 1957). The REBT educational model forms the basis of the establishment of a collaborative working alliance aimed at administering therapy. And for the client to accept the status and move on, he/she needs to be emotionally responsible in addition to owning up to the problem at hand. The client has to come to terms with the fact that life never offers everything we yearn for and happiness is normally diluted by misfortunes that come our way. REBT invites clients to respond in ways that are healthy when their goals seem to be blocked. Alternatively one can react in a way that is unhealthy and unhelpful to misfortunes (Wolfe, 1995). An individual’s way of responding to their blocked goals is heavily influenced by their beliefs. Even though people express themselves differently, beliefs that affect individuals vary according to three common irrational beliefs that all feature demands about individuals, other people, or the world- the basic musts. These compel individuals to do well to win the approval of others as good performers. Moreover, individuals feel that they should be treated considerably, fairly, and kindly as they expect to be treated. And if people fail to treat them as per their standards, they then condemn such people to punishment. Such individuals expect to get what they want, when they want it and must not be given what they do not want.
They can’t stand the fact that there are times when they cannot get what they want when they want it. These beliefs only condemn them to shame, depression, sense of guilt, passive aggression, and acts of violence, they become outrageously stern, self-pity and procrastination. REBT intervention involves engagement of clients by first building relationships with them by empathizing with them and showing them respect and warmth. Secondary disturbances should then be checked. Finally, clients have to be shown that change is possible and it is through REBT that this change can be realized. The second step of treatment involves assessment of the problem, the person, and the situation (Wilde, 2001). This begins with the client’s testimony of what they deem wrong for them. Secondary disturbances should then be checked. The general assessment then ensues to determine the presence of any related clinical disorder. The client’s personal and social history and severity of the problem should then be obtained. Relevant personality factors, non-psychological causative, physical conditions, medications, history of substance abuse are then noted.
The client is then prepared for therapy. But first, treatment goals have to be clarified to ensure that they are concrete, specific, and acceptable to both client and therapist. Introduction about basics of REBT and the biopsychosocial model of causation should be done to the client. Approaches to be used and implications of the treatment should be discussed after which a contract can be developed. Implementation of the treatment program involved analyzing specific episodes of the target problems. Beliefs involved were ascertained, changed and homework developed. Behavioral assignments were then developed to modify ways of behaving. Supplementary strategies like relaxation training and interpersonal skills training were used. The progress of the client with the intervention was evaluated to ascertain whether improvements are due to significant changes in the client’s faculty of thought or just external. One of the problems encountered during the treatment process was telling the client to discard self-esteem and aim for unconditional self-acceptance irrespective of their traits and behaviors. Another significant problem was secondary disturbance which complicated the client’s behavioral and emotional difficulties.
Reference List
Ellis, A. (1957). Rational psychotherapy and individual psychology. Journal of Individual Psychology, 13: 38-44.
Wilde, J. (2001). Interventions for Children with Anger Problems. J. of Rational-Emotive Cognitive-Behavior Therapy. 19(3):191-197.
Wolfe, J.L. (1995). Rational Emotive Behavior Therapy Women’s Groups: A Twenty Year Retrospective. Journal of Rational-Emotive & Cognitive-Behavior Therapy. 13(3): 153-170.